
Note: This piece concerns itself with the social dynamics of COVID-19 and the memetic lag of various psycho-social structures for continental/multiply connected societies. Not islands, like Taiwan, New Zealand, and South Korea. If this statement doesn’t make sense to you, I recommend that you read this piece first.
The above island systems are also interesting — but they need their own piece. I do write some about Taiwan here.
One of the questions on many people’s mind about now is “When will the pandemic be over?” With case counts quite literally soaring, from different testing regimes, it’s a fair question. We’re also bombarded, especially those or us that are educated, to “believe science” or at least “believe scientists.” What that actually means I’ve covered in other pieces. There are no simple answers in this pandemic.
At the same time, every pandemic ends. As I wrote in this piece, the smallpox pandemic that the Aztecs experienced after Cortes exited the scene (to return afterward and conquer their empire) ended with 40% of the population dying. But it ended. It’s no surprise to find that the Aztecs got hit by the double whammy of a new virus (smallpox) plus seasonality that helped spread it. According to Wikipedia, the smallpox epidemic started in May, and lasted through to September of 1520. If you’re up on the literature, this sounds familiar for low latitude countries, that, for a variety of reasons, seem to spread their respiratory viruses over the summer months.
And this virus, too, will end. As I’ve written before, COVID-19, like virtually all viruses, is intensely affected both by seasonality and sociality. Both matter. If you have a super-spreader system like the New York subway, you’re likely to err on the unlucky side (24%) of antibody seroprevalence, whereas if you have less sociality (as in rural America) you have longer periods to build asymptomatic spread and inoculate/variolate your population before the bad season comes. I’ve used the wildfire analogy before with COVID, and it seems to be catching on (though obviously no one read this blog and stole it from me — and I do not endorse all the views in that piece!)
If you ignore the sound and fury associated with recent case counts — do remember that testing is awful (this is one piece, but there are so many of these it’s mind-boggling, yet still under-emphasized,) it’s uneven, the numbers are conflated, and it’s really only championed by empirical scientists that hang their hat on that kind of thing, as well as their followers, there’s really only one gold standard of statistic that matters. And even though THAT is weak (we have no idea of the various conflations going on regarding whether someone who died was on death’s door, and just happened to get COVID at the last minute) I’m standing by COVID death counts as our tarnished measure.
And that is interesting enough. Take a look at Canada, for example. What do you see?
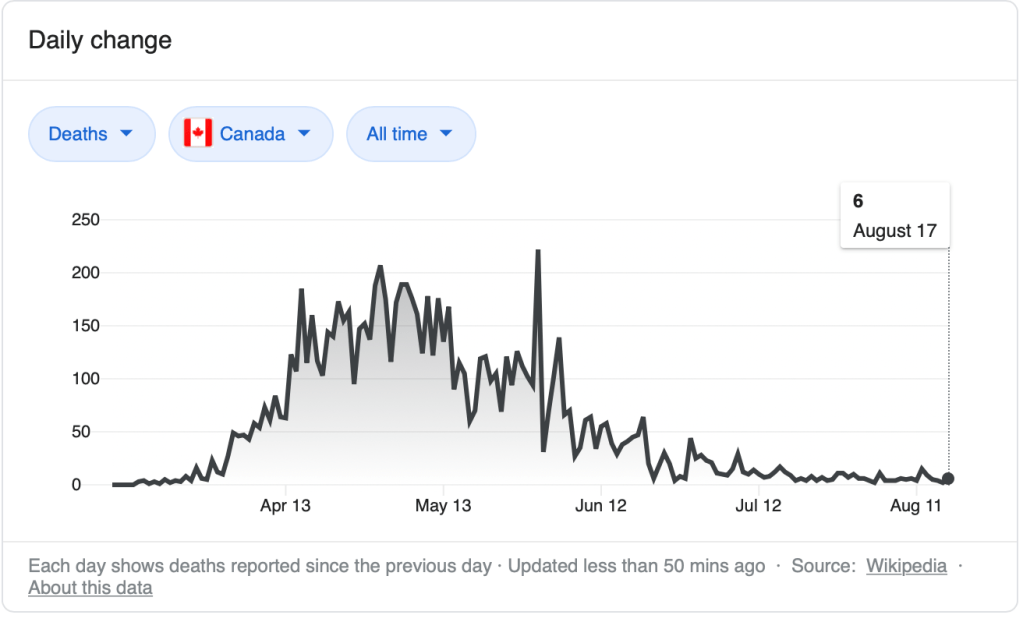
What you get to see is that the pandemic is functionally over in Canada. And while there are still the COVID-doomers in both the government and on the sidelines touting increased case counts, the reality is that this thing is over. Officials in Canada who were previously hollering for tighter measures, a month after deaths have gone to zero, are backpedaling. Canadians are also tired of social restrictions, and are demanding a return to a more open, empathetic society.
It’s instructive to look at Sweden as well. Their death plot looks like this:
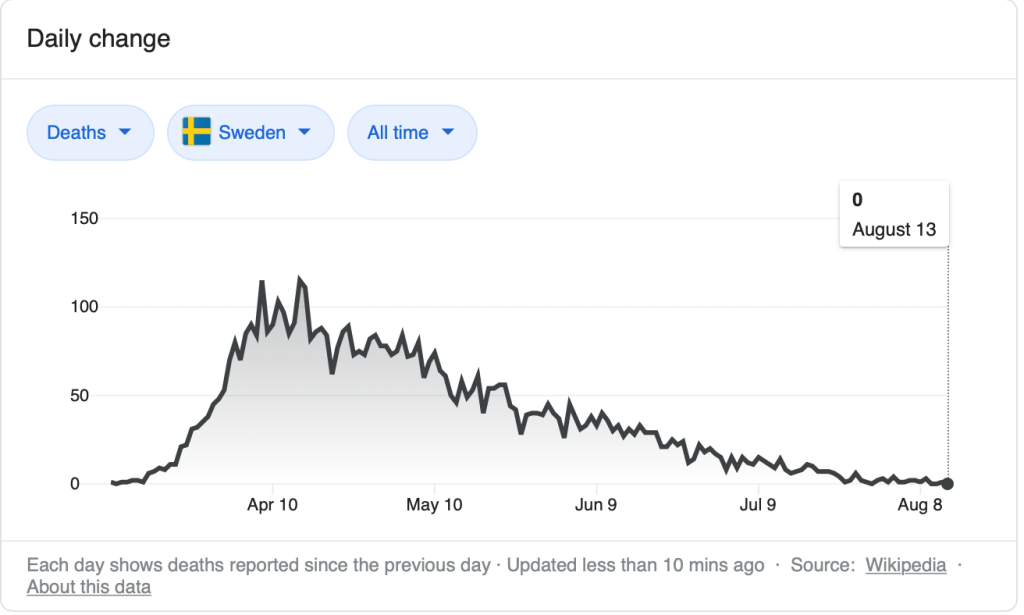
Sweden was the nation that pursued a moderate course of action of social distancing, closing some schools, and other agency-based, voluntary restrictions with the idea that the society could move to herd immunity. Scientists in the Swedish public health authority ran the pandemic response independent of Sweden’s political government. The end result was that, of course, there was no lag at all between the population and leadership. It is true that the leadership did make mistakes, especially regarding the management of care homes. But in the end, Sweden passed through, and now has virtually no COVID cases.
I’m including Spain — another example of a modestly Authoritarian yet still a parliamentary democracy — for reasons I’ll share below:
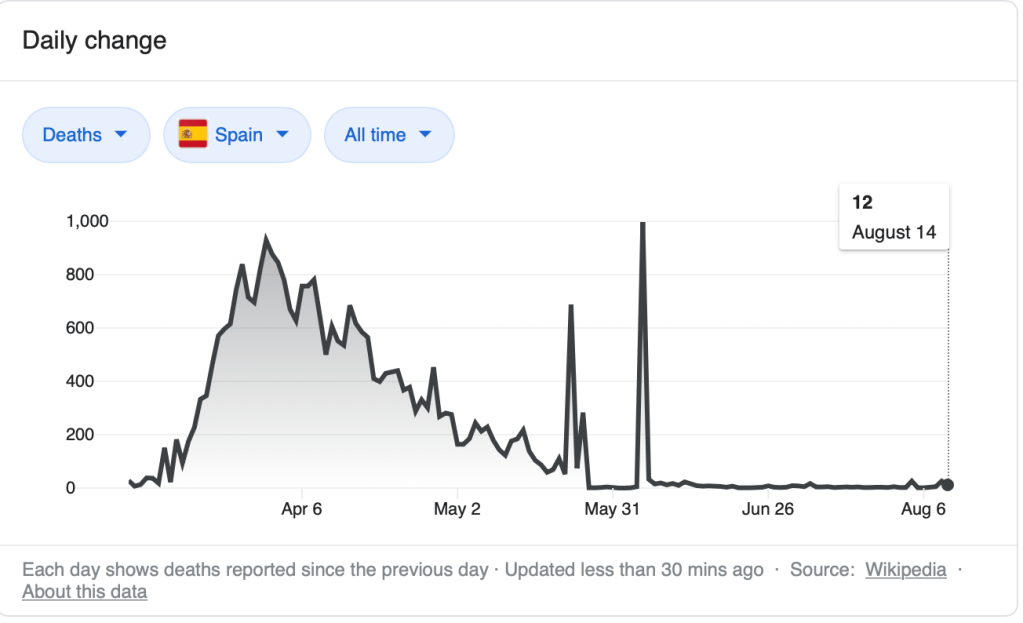
Though there seems to be reconciliation happening (see the spikes!) in the numbers used to produce these graphs, it’s pretty clear that Spain (even with all that sunshine) is a Northern Tier country. Its pandemic was over at the end of May, and all plots I’ve seen comparing Spain to other countries indicate Spain in the upper end of effectiveness (if there really is such a thing) in COVID prevention.
One thing that is amazing is how the media enforces the COVID control narrative. This should come as no surprise — reporters are often belief-based and status-driven, and status of sources matters. You don’t maintain high-status sources by making them look bad. So if the authorities say the pandemic isn’t over, well — the v-Memes will do the talking. But some people — in the case of the video below, a doctor — are confronted with what I call grounding validity. They’re sitting in the hospital, looking at their bed stocking rates. And they have opinions. The video below is stunning in watching how that very grounding validity works against the status-based social structure of far too many contemporary journalists. Highly recommended.
As I’ve said before, I am a fan of Ivor Cummins, on Twitter as the @Fatemperor. Ivor’s in Ireland, a nutrition specialist and ex-liaison engineer that I’ve written about here. And Ivor’s not very happy about the fact that Ireland’s death total has gone to zero now for 2.5 months, yet people are still calling for lockdown. Here’s their death curve.
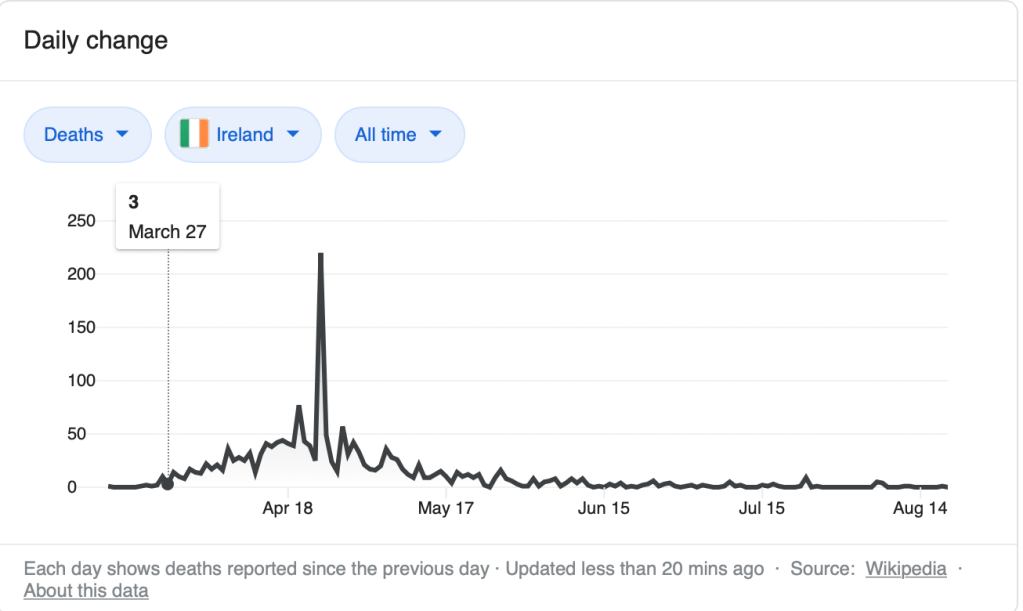
What does it say about the psycho-social development of Ireland that its politicians are demanding lockdowns when the pandemic is so obviously over? Nothing good about empathy. And lots about the residual authoritarian Catholic culture of control.
Now let’s talk about the United States.
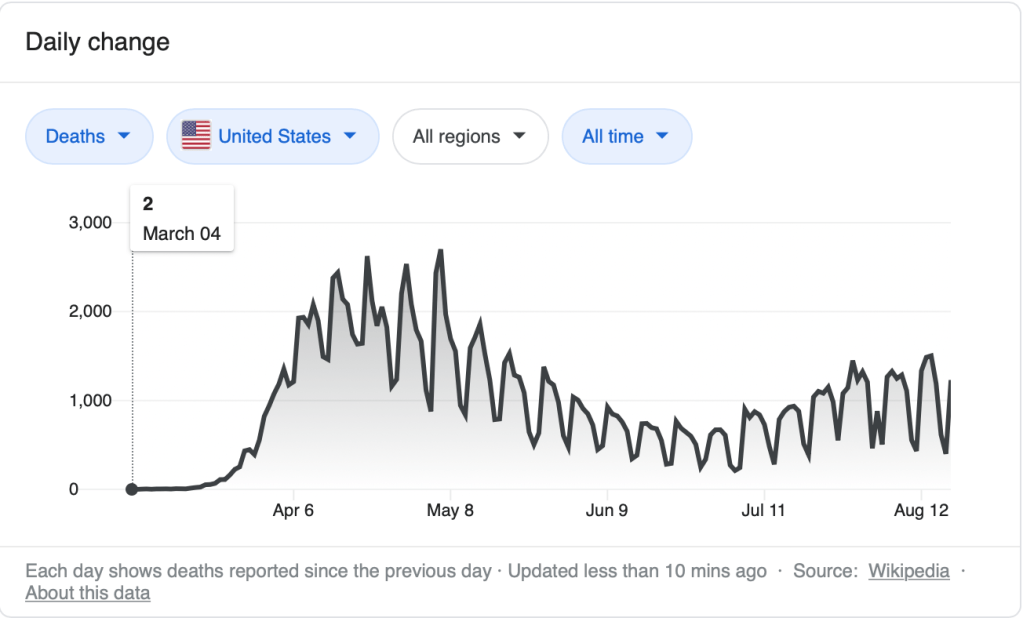
As I said earlier, COVID spread is a combination of seasonality and sociality. The seasonal aspect shows up in the US in two ways — the northern tier big bump came, peaking in April, and augmented by our super-spreader system called the airline system. The southern tier is following similar seasonal dynamics of low-latitude countries, with some type of peak mid-summer. This type of behavior can be seen in other countries as well, regardless of human intervention. Peru had a severe lockdown, but is demonstrating a similar curve. Colombia, less so, but the same pattern.
Sociality can make a difference, and also matters in the US — I saw an analysis of New Orleans around Mardi Gras — a big spike coming from the influx of travelers. But then things died down until seasonality came back in the early summer.
In the US, none of our authorities explain any of this with any sense of consequentiality. Instead, what we hear are shaming messages if we don’t agree, and overt politicization of the pandemic. I’ve written over and over that what causes pandemics to be held at bay is a.) coherence of action of the population, as well as b.) timing of interventions. It doesn’t do much good, for example, to have a lockdown once the bug has already spread.
What is more interesting to me is the messaging regarding, as well as time delays for admission that the pandemic is over, is the evidence that it gives for what type of v-Memetic system is in place inside a country. We can see Canada has maybe not the perfect system, but in the face of more rigorous measures, the people push back when the evidence isn’t there — consider them solid Communitarians. The Swedes straddle the Communitarian/Global Systemic boundary — they have the ability to take responsibility for individual actions, and at the same time hold fundamental principles of liberty as more important than the mistakes of their experts. High social cohesion also helps, and hearing public officials reflect on some of the failures demonstrate that Global Systemic v-Meme.
And what of the U.S? I’ve been following John Robb’s work lately. He’s got a great term called ‘networked tribes’ — and I’ve written about the dichotomous binning of information that has deeply affected the politicization and weaponization of the pandemic. When will our pandemic be over? It will end. But because of our v-Memetic discord, and the Networked Tribality of our message, it’s going to take a long time.
What’s the upshot of all this? Short version — pandemics are a time-dependent phenomena. This one’s been going on in the West since February for sure, peaking (dependent on latitude) in the North in April, and in the South in the middle of the summer. That’s clear from the graphs of data we sadly, actually know — people dying. The lag between people acknowledging that it’s actually over is, at some level, a memetic response of the system. The more authoritarian our system is, the less desirous it is of restoring empathy and giving up control, even in the face of clear evidence.
And here’s the deeply distressing thing. What does it mean when our system, regardless of political party, refuses to give any other interpretation to the pandemic other than we should never live a normal, free life again, under pain of death, while at the same time pushing past control actions and narratives that can be shown, through evidence, validity grounding and critical (and often complex) thought, not to work? I leave that one to you to ponder.

I’ve been arguing for a more local approach for a while now. In the United States, this would not even mean primarily on the state level but much more local in terms of counties and cities. In the case of large cities, different responses might need to be done at the level of neighborhoods and individual schools, organizations, etc. Allow more democratic process in local citizens and officials deciding what policies are implemented based on local data and local concerns.
Throughout this public health situation, some populations were almost entirely unaffected while others were being devastated (on one Native American reservation, 6% of the population tested positive and about 1% of the population died). Even now, some places have seen infections drop extremely low and yet in other places infection rates spiked with reopening of schools. Talking about national public health policies is probably unhelpful. Responses should be to specific conditions in specific places.
I have no grand opinion other than wait and see. Schools are just now reopening and so we won’t know the results until the coming weeks. That isn’t even to discuss possible later waves of infections, hospitalizations, and mortalities later in the year when northern populations are low in vitamin D and if a tough flu season hits, a set of conditions that is unpredictable in outcome, especially as viruses can mutate as happened in the second wave of the 1918 flu. It seems most communities, institutions, and businesses should reopen.
Yet we should continue practicing risk reduction until it’s clear that infections are permanently dropping. We’ll only know it’s over for certain in retrospect. Past pandemics went through multiple waves and this one may do so as well. Then again, infection numbers could remain low. No one knows and no one should pretend to know, even as there is nothing to be panicked about at the moment. I wouldn’t be dismissive of continuing concerns, in particular for populations that remain at higher risk because of greater rates of immunocompromise, comorbidities, and lack of healthcare.
More than anything, we should have fair and honest news reporting and public discussion about the data. Then based on that, we should openly consider what this means going forward, as data might change.
LikeLiked by 1 person
Here is the main thing that has bothered me from early on. I dislike the polarized debate of it all. It is magnified by partisanship, but it’s broader than that. Right from the start of it, many quickly formed two sides, one arguing it’s like the common flu and the other arguing it’s the Plague. There was no nuance to public debate, much less a middle position or (God forbid!) intellectual humility.
My main response has been cautiousness, as based on the precautionary principle. It’s my standard response to most major issues, such as climate change. It’s better safe than sorry, at least when dealing with potentially deadly or otherwise destructive scenarios. Yet it’s hard to know what is reasonable and wise cautiousness under unknown conditions, although it’s precisely such a situation where the precautionary principle is most applicable.
The novel coronavirus is aptly named. It literally is not like the common flu, since it’s an entirely different category of virus. But it obviously doesn’t act like other coronaviruses we are familiar with such as the common cold. It quite possibly was altered, if it’s true that it escaped from a Chinese lab. All of the uncertainty comes with the territory. That is the nature of pandemics, they are unknown quantities. We never know when they’ll come, how they’ll develop, or when they’ll end. That is because viruses are so unpredictable and easily mutate.
It’s hard to know how to create public policy for a pandemic. Even in the middle of this crisis, we still aren’t quite sure what to do. Nor can we agree to something as simple as where exactly we are in the crisis. I’ve seen some argue that we’ve already been in a second wave and it’s winding down. But experts I’ve heard say we are still in the first wave, just temporarily suppressed during lockdown. Others agree that this is the first wave and it’s ending now. Yet some point to particular places where infections have spiked again with reopenings.
We can look to past pandemics. The most comparable, of course, is the 1918 flu. It had three waves with the last happening the following year. It started much like Covid-19 in being mild. Many dismissed it early on and there was the same struggle over public policy, including people refusing to wear masks. The similarities are almost shocking in demonstrating how little humanity learns from past experience. The first wave dissipated without much harm or death, just like the present first wave of novel coronavirus, but the virus later mutated and came roaring back. It was only in the second and third waves that millions died.
Other pandemics also have had multiple waves or have extended over multiple years, sometimes with recurring waves over decades or centuries. That is a common pattern. So, there is no particular reason to assume that our present pandemic will end with a single wave. One thing we can be fairly certain about, if there are later waves this year and heading into next, there is possibility they could be worse in being more infectious or more deadly. That is because of the specific contributing factor of vitamin D deficiency in fall and winter, and hence exacerbated immunosuppression in a population that isn’t exactly immunologically healthy.
That is why, as you know, flu seasons happen that time of the year. And so it’s the reason why a second coronavirus wave would likely coincide with flu season. Furthermore, multiple infectious viruses simultaneously would have different health effects than any single infectious virus alone. That means the unpredictability increases. Coronavirus infections could peter out and not come back or linger at a low level without further concern. Even a second wave wouldn’t necessarily be at pandemic levels, as a repeat of the pattern of certaub past pandemics. The fact of the matter is simply that no one knows. Yet so many people are talking with so much certainty. We are still in black-and-white thinking, either mass deaths are on their way or it’s completely over.
Think back again the 1918 flu. How different it is to look at it in retrospect than to live through it. We think of it as the most major pandemic in modern history. Yet in the first wave, it was so mild as to kill few people and be easily ignored. As with right now, people were focused on other things, in that case with a world war going on. People get tired of worrying about Covid-19, and the media has a short attention span. How quickly nearly all talk of pandemic disappeared during the BLM protest movement and now with the present storm damage, wildfires, etc. And the presidential election will also likely turn our attention to other issues as well.
Most people are ready to move on to something else, and one can sense the still ongoing debates losing much of their steam. It’s irrelevant what anyone thinks at this point. We’ll move forward as a society and the novel coronavirus will do its own thing irrespective of our decisions and concerns. It’s almost pointless to even talk about such things as possible second waves, as it either will happen or it won’t. If a second wave does happen, we will be unprepared for it because we wouldn’t know how to prepare for it and we don’t have the political will or economic capacity to do a second shut down.
No matter what happens next, we will simply have to plow forward and hope for the best. There is no point in worrying about it. We may reached the furthest extent of the precautionary principle under the crippling conditions of this dysfunctional society. The same goes for climate change. Whatever will happen will happen. The time to prevent or prepare for such crises was decades or generations ago. Besides, it’s unlikely we will learn any lesson from this, any more than the past experience of the 1918 flu helped us know how to deal with the novel coronavirus. As a species, especially in this country, our ability to deal with mass catastrophes and crises is pretty much limited to reacting to them. That is unlikely to change.
All the analysis and debate is moot, even if we had good data and were able to understand what it might mean. By the way, Chris Kresser has a good rundown on the present moment of Covid-19 (https://email.chriskresser.com/assorted-links-covid-immunity-masks-schools-testing). He points to some evidence that maybe herd immunity could actually happen, as elusive as it has seemed — let us hope that finally happens. But the bigger concern, that I’ve been ranting about for months, is what he refers to as “Long COVID-19”.
Herd immunity might come at a high cost. And that cost in personal suffering and healthcare spending could extend far into the future. Once again, no one knows. That is to say, a wise person would not be seeking to get infected in the hope of getting closer to herd immunity. The most rational course remains to reduce risk while waiting for the possibility of a vaccine in the near future. In case you’re interested, here is the piece that Kresser links to (https://www.theatlantic.com/health/archive/2020/08/long-haulers-covid-19-recognition-support-groups-symptoms/615382/):
“A few formal studies have hinted at the lingering damage that COVID-19 can inflict. In an Italian study, 87 percent of hospitalized patients still had symptoms after two months; a British study found similar trends. A German study that included many patients who recovered at home found that 78 percent had heart abnormalities after two or three months. A team from the Centers for Disease Control and Prevention found that a third of 270 nonhospitalized patients hadn’t returned to their usual state of health after two weeks. (For comparison, roughly 90 percent of people who get the flu recover within that time frame.)
“These findings, though limited, are galling. They suggest that in the United States alone, which has more than 5 million confirmed COVID-19 cases, there are probably hundreds of thousands of long-haulers. […]
“Putrino thinks that many long-haulers have symptoms that resemble dysautonomia. This is an umbrella term for disorders that disturb the autonomic nervous system, which controls bodily functions such as breathing, heart rate, blood pressure, and digestion. Damage to this system, whether inflicted by the virus itself or by an overly intense immune response, might explain why many long-haulers struggle for breath when their oxygen levels are normal, or have unsteady heartbeats when they aren’t feeling anxious. Things that were once automatic are now erratic.
“More than 90 percent of long-haulers whom Putrino has worked with also have “post-exertional malaise,” in which even mild bouts of physical or mental exertion can trigger a severe physiological crash. “We’re talking about walking up a flight of stairs and being out of commission for two days,” Putrino said. This is the defining symptom of myalgic encephalomyelitis, or chronic fatigue syndrome. […]
“But COVID-19 is still a new disease, and ME/CFS is just one of several possible outcomes. Some long-haulers recover before the six-month threshold. Some don’t have post-exertional malaise. Some have lung damage and breathing problems that aren’t traditional ME/CFS symptoms. Some have symptoms that more closely fit with other chronic illnesses, including dysautonomia, fibromyalgia, or mast cell activation syndrome.”
LikeLike