Though, of course, I find it difficult to escape my own frame on writing about issues — I can’t resist peeking under the memetic hood of this crazy civilization we’ve created — I’m going to try with this post. No promises, though.
We’re now 10 months or so (give or take who’s counting) into this pandemic — and largely, the people that have borne the cost of our fears are our children. Kids have been displaced out of schools due to COVID fears, and Very Important People, while even attempting to leaven their messages and tell officials to keep schools open (who would better come to mind than Gov. Gavin Newsom and Dr. Tony Fauci?) keep the overall fear-o-meter pegging against the charts. That hardly helps anyone understand exceptions, or spread, or really anything. We’ve established the largest full-scale suspension of freedoms with nary a vote in our lifetimes.
And what has it gotten us? If you look at the data, very little indeed. The most recent COVID death chart from the U.S. is posted below. It’s what we engineers call a time series — a plot of COVID deaths over time — and while the artifacts (the sawtooth waveform) are due to a number of reporting issues, the deep reality is that there is no place on that curve where a systems engineer might point to and say “hey — this is where our social measures made a difference.”
Well, anyone that’s honest. Here’s the plot.
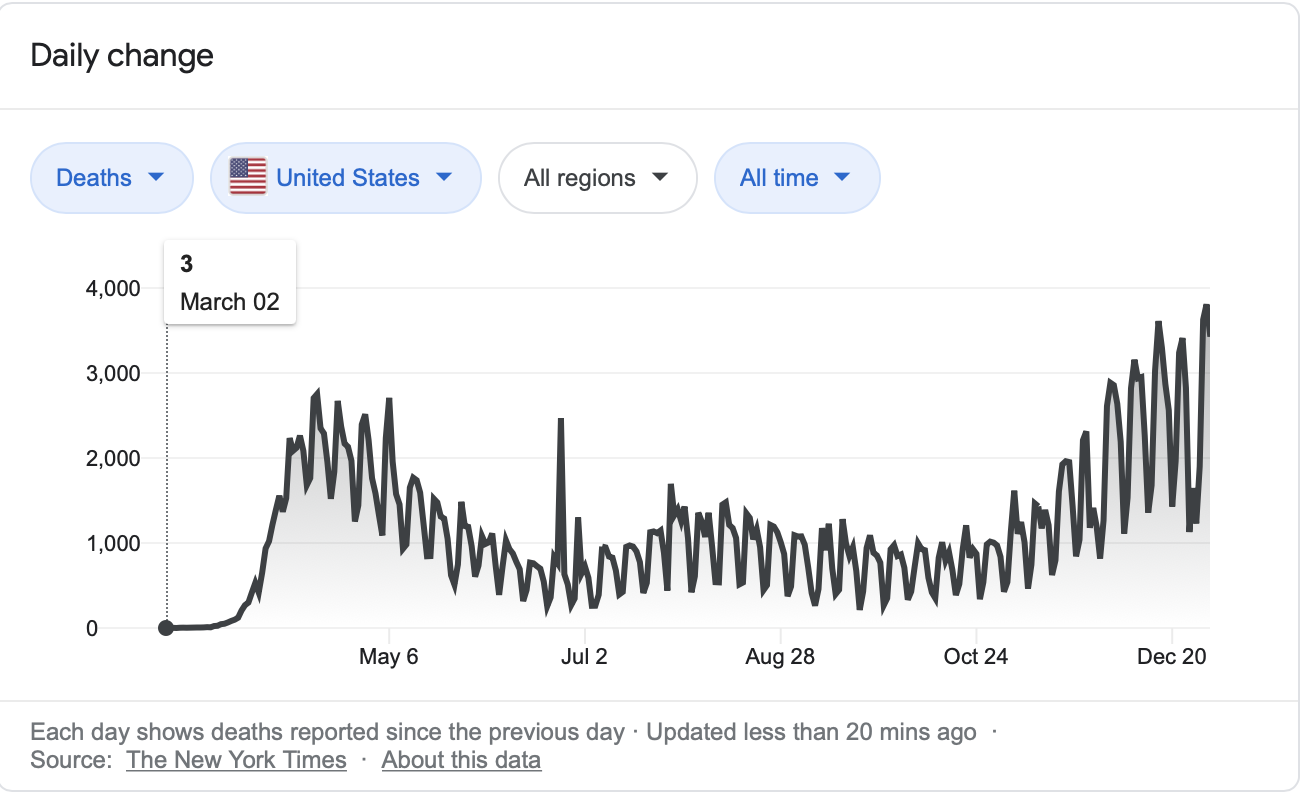
You can’t look at that plot and honestly say “see — this is where we made a difference because a majority of folks started wearing masks,” or “this is the result of our Thanksgiving Holiday Super-spreader Event.” There’s a little bobble through the points in the Christmas holiday, but what they average out to is a bending over of the classic respiratory illness death curve that characterizes the pandemic.
The shape of the overall curve is actually far more understandable than is made out in the media. COVID showed up late, and on the shores of the US in February, and in the tailwind of a weak respiratory illness season in 2019, gave us the big punch up in numbers in high-latitude, low elevation country in the US in March and April. This was followed by the typical low-latitude surge in the southern states in the summer, and the green field COVID wave I call the High Plains/Upper Midwest surge that happened in October. Then the country settled down into its usual seasonal pattern (what we’re experiencing right now) with COVID beating flu to the punch. We’re at the descending peak of that wave now.
Why any of this is a surprise is beyond me. The structure of the pandemic mirrors insights already created by people like Jared Diamond, in ‘Guns, Germs and Steel’ — where he famously laid out the key indicators of disease vectors as aligning, in simple latitudinal ways in Eurasia, creating more domestic animals and disease resistance. This vs. the North/South alignment of the New World. Our climatic variation has always been the thing that has governed life on this side of the pond, and it’s no different now.
And even discarding that Big Picture insight, the reality is that, well, not much changed with all that we have done. Yes, it is impossible to say, because we don’t have a “control” country to run an experiment against. But if you just look at the modelers’ data, they have consistently over predicted the event as a calamity of historic proportions. Which, well, it’s not. It’s a bad time, but it doesn’t come close to the real pandemics of the past. It is utterly mind-boggling that these models, having been so chronically wrong, are paid attention to at all. History will not be kind to the recount of those efforts.
Over and over, we’ve attempted to pin this pandemic on those we disagree with politically. I’ve written about this here. It’s just nuts, and these things have to stop. Or we’re going to end up in a civil war. And that will kill far more young people than COVID ever could.
Where we are missing the boat regarding COVID is the damage that the pandemic has done through destruction of relational growth that really fuels how young minds are formed. Primary- and secondary school-age kids get this from going to school, and there is no real risk, despite the histrionic anecdotes pushed by the media, for school children. Yes, there is a smattering of extremely tragic cases that are part of the pandemic. One of the curiously sociopathic angles discussing COVID is the risk to football players for some version of myocarditis as an after-effect of the pandemic — as if the well-established dangers of smacking each other’s skulls together weren’t enough. There can be no better juxtaposition of how we perceive risk, however. One is a reason to lock down/up our children indefinitely. The latter is merely a continuation of “how we do things around here.” The various lockdowns have been done ostensibly to save the old, though, once again, it’s not clear that any of this anti-socialization has helped them either. In fact — probably not.
When it comes to college-age kids, living in a university community, I hear the constant berating from the elders about irresponsible college kids are, because they continue to socialize. And it’s wild to me that voices of control have been recruited from the student population themselves. I’m not going to name names, because I still have hopes that these young people, though adults, will grow out of the need to please their elders and represent their natural constituencies. There is really functionally no risk to college kids as well. And schools that have opened (I live next to the University of Idaho) have managed to even control spread, as much as it can be contained, than schools that have gone online. Which would, not surprisingly, jibe with the overall statistics — that not much we’ve done, plus or minus, really matters.
If we’re to start understanding why the enforced collapse of socialization matters to all students, we’re going to have to come to terms with what we actually do in schools. The answer is not “we smart adults tell students a bunch of stuff, they soak it all in, and they’re far better off for it.” I’ve been teaching (and winning awards) my whole career for teaching, which is really only a modest part of a relatively modest career. The reality is that students learn mostly from each other. And the lessons they learn, sometimes sweet, sometimes bitter, are mostly about how to relate and listen to each other. We sprinkle the lessons of the venue on top of all of this, of course. But the biggest hunk of everything they learn involves themselves, and their interactions.
My tagline, since I started my empathy project, has been “as we relate, so we think.” The meaning of this is not simply “if you relate nice, then you think nice.” The stakes are far higher. The DeepOS lesson of all this is that relating to different people, across varying ages, social statuses, and racial/ethnic variations, creates the conditions in the brain for other complex, more discipline-specific information to get slotted. Without that interaction, though, the brains of young people, while not exactly being frozen, do not thrive. And being that all people, in all walks of life, are spread out on a probability distribution for pretty much any issue/concept you can think of, we will decrease a certain percentage of the population’s intellectual and developmental abilities in ways we cannot predict yet. If you say you care about disadvantaged populations in the U.S. this should deeply concern you. Those will be the students whose starting line is moved back once again. My advantaged students, and their parents, can and will find ways around this, and I absolutely do not begrudge them.
But in a time of already-extreme separation between opportunities for rich and poor, those without resources, juggling even furnished iPods in mediocre online classrooms, will be even more screwed. Don’t fool yourself. And they also will not have the more evolved social environments that well-off parents are already creating for their children. Mores the pity.
Just so folks know, I’ll be back in the classroom myself in 18 days, running students through my curricular vehicle, the Industrial Design Clinic. I’m one of the few that’s made that choice. It was not forced on me by my administration. And, no, I haven’t had the vaccine. And yes — when I’m told my number’s up, I’ll get in line, but not before. I already know there are people that need it worse than me. There’s a reason I have 2400 hours of sick leave accumulated through my career– it’s not because I’m unhealthy.
I’m doing it because, even though it will be a difficult classroom environment, it will give my students to get to know their best teachers — each other. We’ll be in masks, we’ll be wiping down tabletops, all things of indeterminate efficacy, but part of whatever set of rules we are told to follow. But we’ll do it together. And I’m looking forward to a great year.

What your graph reflects most clearly is the incoherent mind of Donald Trump, not the effectiveness of any strategies. Other nations have had fantastic success – authoritarian China (lockdowns, quarantines, track and trace) and democratic Taiwan (quarantines, track and trace, tight border controls) being two. In the UK the first lockdown was very effective at temporarily reducing deaths – the later Tier system less so, as can be seen in the charts at coronavirus (dot) data (dot) gov (dot) uk/details/deaths. Our Track and Trace system is a joke.
In the UK, once the initial panic over vast numbers of deaths had passed, attention seems to have turned to the collapse of the health service – a very different matter. Even a small increase in the number of very severely ill AND infectious people can tie up intensive care beds and staff and clog up the rest of a hospital. Roughly speaking, 50,00 people a day test positive in the UK, 2000 people a day enter hospital as a result of COVID, and 400 die (coronavirus (dot) data(dot) gov (dot) uk/). Those that enter hospital are probably going to be there for between one and three weeks. Although such patients are only a relatively small number it’s enough to bring critical care services to the point of collapse and to slow everything else down to a crawl. The critical care doctors we see daily on T.V. make it very clear how desperate the situation is for them and how exhausted they and their colleagues are.
An attempt was made to increase critical care capacity by building the ‘Nightingale’ hospitals. This was before the realisation that COVID is a mutli-organ disease requiring input from multiple professionals, best found in conventional hospitals. The Nightingales consist of beds and ventilators, but without the appropriate staff are effectively useless for what they were designed for.
The effectiveness of masks is debatable but as a psychological strategy bringing home the message that these are not normal times they probably have a certain effectiveness.
LikeLike
This comment is half-meaningful, half-ridiculous, and rebutting the ridiculous stuff takes more time than I care to put into it. This is a blog for insightful people — in the future, I’ll just delete comments like this. You can find plenty of audience on the large social media platforms. If you want to understand Taiwan (an island) and China (an authoritarian nation with a large propaganda arm), here are some insights.
In the future, I’ll just delete your comments that don’t respond to the arguments in the piece.
LikeLike
Just discovered your site in April 2026 and have been reading it for the last 5 hours or so. Excellent work! Truly impressive! Now that so much time has passed, I am wondering if you regret taking the covid vaccine? As for me… I knew covid was a scam as soon as I saw the Event 201 videos – that is to say – before it even started. I printed up bumper stickers of a masked face with slogans such as “child abuse”, “i hope this never ends,” “i live in fear,” and “i will obey,” etc. My son was born in November of 2019 and then vaccine injured in April of 2020 after his 6-month doctor visit because only 1 parent was allowed inside due to covid and my foreign born wife was pressured into over-vaccinating him that day with a flu shot on top of the regularly scheduled jabs. (he was just diagnosed with autism at the age of 6… they really like to put some space between the 2 events so they can deny the OBVIOUS connection.) The good news is that by mid-2000 I knew I was NEVER allowing anybody in my family to ever be injected with anything ever again, and my absolute distrust of institutions was at an all-time high.
Here is an entertaining story that for me really defined the mass psychosis and utter idiocy of the population during covid: My wife and infant son and I went out to eat one night. I showed the hostess the fake vaccine cards I had printed out. She pointed the little gun at our heads to take our temperatures… and my baby was running a little hot. I watched these masked retards jump back in horror from him like he was a pipe-bomb! It is very sad that so many people were stupid enough to fall for the covid scamdemic and inject themselves with an untested vaccine that caused countless cancers, strokes, and heart attacks. It wasn’t a pandemic. It was an intentional depopulation event. But most of all It was an IQ test. The deaths in 2020 were mostly due to the deadly treatment protocols in the hospitals. The real rise in all cause mortality started after the vaccines were released. I strongly suggest you check out escapekey.substack.com if you really want to understand the matrix we are living in and the global control systems the “elite” are implementing at this very moment.
LikeLike